Since receiving my endometriosis diagnosis in November of 2017, I have researched, educated, and advocated for better and proper endometriosis care. This, of course, stems from the fact that my first surgery was unsuccessful and significantly worsened my pain and symptoms. It wasn’t until a year after my first surgery that I realized that I did not receive the gold standard in endometriosis care: Laparoscopic Excision by an expert excision specialist. Instead, I received the more utilized technique commonly referred to as endometriosis ablation, but also known as fulguration or cauterization. So today I will answer the question . . . Does surgical method really matter?
Does Surgical Method Really Matter?
Endometriosis Excision vs. Endometriosis Ablation
Endometriosis Excision
Because endometriosis is incurable, symptom control and improved quality of life remains the goal for endometriosis warriors. Currently, the gold standard to proper diagnosis and treatment is laparoscopic excision surgery.
Laparoscopic excision (LAPEX) surgery is a key-hole surgery that involves the use of a heat energy to cut out the endometriosis tissue, including the tissue below the surface. This method is the gold standard because its goal is to remove all endometriosis lesions, while supporting organ function and avoiding destruction of the surrounding healthy cells. It also allows for the excised tissue to be sent to pathology for confirmation of endometriosis.
The biggest benefit to LAPEX is that it gives patient the best chance for remission, as it provides “long-term relief in 75-85% of [endometriosis] patients (1).”
Unfortunately, few surgeons are trained in excision of endometriosis. To date, physicians are being taught outdated methods, treatments, and theories when it comes to endometriosis. This leads to years of misdiagnosis and suffering for those of us living with the disease.
Endometriosis Ablation
Instead of referring patients to excision specialist, many Ob-Gyn’s continue to use laparoscopic ablation to treat endometriosis. This approach means that they burn the superficial tissue to kill the cells, which leaves no possibility for pathologists to confirm endometriosis. This method can lead to damage of the surrounding tissue and it often leaves behind deep implanted endometriosis lesions that is not visible on the surface.
Yes, ablation is often used in all surgeries (to stop bleeding), but it’s important that the surgeon not use it as a means for endometriosis removal. Because, in the end, the patient will likely have worse pain than before the ablation surgery (something I know about all too well).
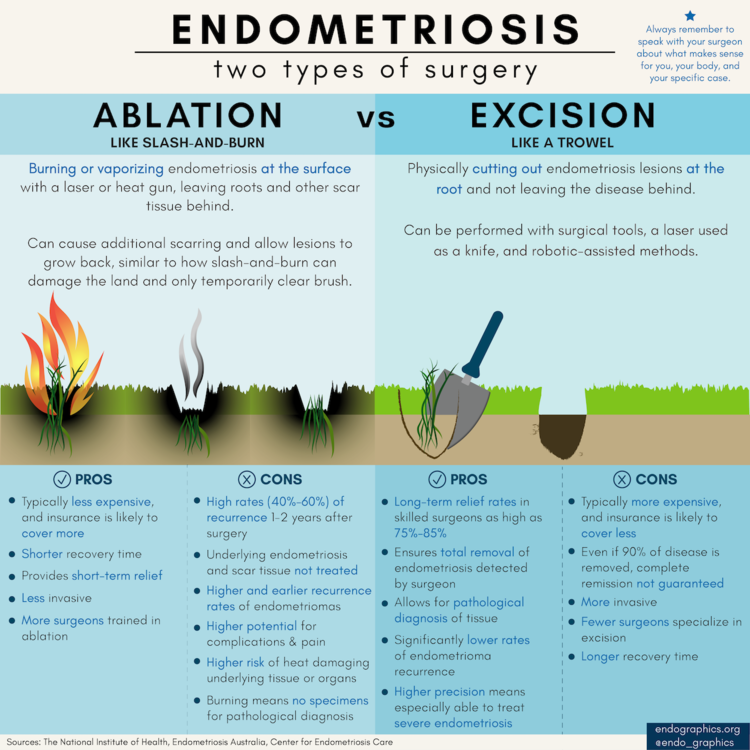
Below is a perfect infographic from endographics.org, showing the differences between endometriosis excision and ablation, as well as the Pros and Cons of each.
What about Laser Surgery?
Many surgeons advertise that they do endometriosis excision and emphasize their skill in robotic laser surgery. But it is soooo important that you recognize that the laser is only the tool, and not a sign that they are a skilled excision specialist.
The laser is the tool, but the method in which the tool is used is what matters. The laser can be used to excise, or it can be used to ablate endometriosis. So, it is really important that you interview your surgeon and find out what method they use.
The most common type of laser used for excision is a CO2 laser, but this type of laser can be used for ablation as well. So, again, ask your surgeon what type of laser they use and how they use it.
Even more so, “It is important to understand that [the] tool and method are not nearly as important as [the] skill of the surgeon: if he or she cannot excise, they cannot excise using any method or tool (1).”
Surgical Method and Experience